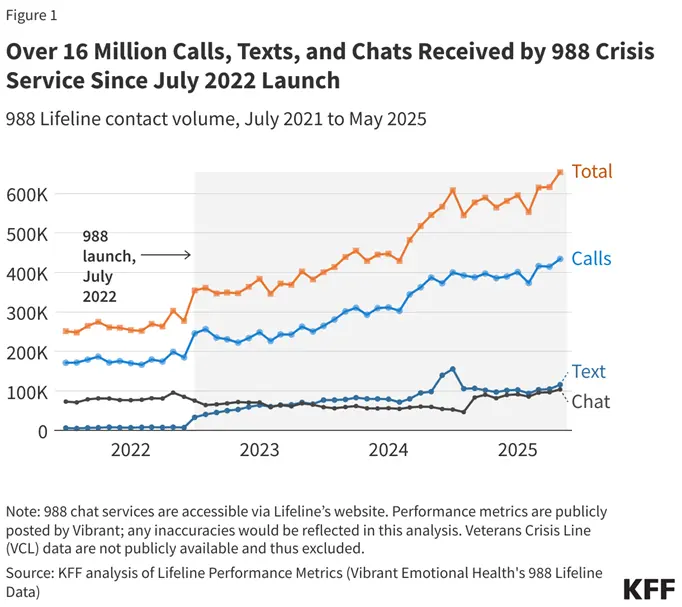
The 988 Suicide and Crisis Lifeline has been one of the most successful systems to help Americans in crisis. In 2025, 988 received over 8 million contacts from individuals through phone calls, texts, chats, and ASL videophones. While it is critical for a support system to be in place for people in need to get help, it is only the first step in the process.
Crisis care expectations are rising, and individuals need help after the initial contact to find the services they need. This idea is called a no-wrong-door workflow. In this article, we'll unpack what that means and how to utilize improved crisis-to-care systems to save lives.

Why Behavioral Health Organizations Cannot Treat Crisis Response as a Standalone Function Anymore
The challenge goes beyond answering a crisis call. Teams must make sure the person gets connected to the right next step, documented properly, followed up with, and kept from falling through the cracks. Only 24% of mobile crisis teams use EHRs (electronic health records) for information sharing during care transitions, showing the information gap that frequently happens.
Crisis response used to be treated like "show-up, de-escalate, and leave." Now, successful behavioral crisis response requires more nuance. People in behavioral health emergencies should receive a behavioral health response, not police by default when there is no immediate safety risk. That response should connect to ongoing care and 24/7 services. That means crisis work must interface with:
- Call centers
- Law enforcement
- Emergency departments
- Peer support
- Housing
- Treatment capacity.
Certified Community Behavioral Health Clinics (CCBHCs) and other behavioral health teams need electronic systems to track continuity, referral completion, follow-up, and documentation across these different stakeholders.
What No-Wrong-Door Access Actually Means in Behavioral Health
A no-wrong-door workflow means that a person can enter the behavioral health system at any time — emergency room, primary care, community clinic, school, crisis line, or behavioral health agency — and still get connected to the right service or referral without being turned away.
As an example, the Los Angeles County Department of Mental Health offers Alternative Crisis Response services that include the following four-part flow:
- Someone to Contact: They offer a 24/7 help line and link to the 988 Suicide and Crisis Lifeline.
- Someone to Respond: They have field intervention teams for in-person support during a mental health crisis.
- Somewhere to Go: Psychiatric Urgent Care Centers are available for short-term stabilization and on-the-spot assessment, therapy, and medication, as well as links to crisis residential treatment programs.
- Somewhere to Treat: Follow-up teams keep track of clients for ongoing treatment, urgent appointment scheduling, and support after a crisis.
This established framework for state and local agencies helps implement no-wrong-door access.
Where Crisis-to-Care Workflows Break Down Today
Crisis-to-care workflows usually break down at the handoff points: when a person is moved from the crisis line or mobile team to a receiving site, from the ED to psychiatry, or from stabilization back to outpatient follow-up. Those transitions are vulnerable to disconnected notes and unclear responsibility, which leads to weak handoffs and delays in the next appointment or placement.
The common challenges for mobile crisis response workflows include:
- The handoff breaks after the initial crisis contact: People get assessed or referred, but the next service is not confirmed, and the case loses momentum.
- Referrals go out, but the loop never closes: Teams often do not know whether a referral led to an appointment, a completed intake, or no connection at all.
- Follow-up is manual and inconsistent: Without reminders, scheduling, and case visibility, high-risk follow-up becomes easy to miss.
- Systems are fragmented: Call notes, assessments, case notes, referral tracking, and billing live in different tools, creating duplicate work and blind spots.
- Documentation and billing are disconnected: Even when care is delivered, poor documentation continuity creates delays, denials, and administrative burden.
Organizations can turn to modern closing-the-loop workflows to address these issues and ensure that no clients slip through the cracks.
The 5 Capabilities Behind a True Crisis-to-Care Workflow
A crisis-to-care workflow moves a person from initial crisis contact to stabilization, referral, and ongoing follow-up, keeping care connected and accountable. In behavioral health, it is designed to help teams assess risk quickly, route the person to the right support, and make sure the next step actually happens.
Here are the five pillars your team needs to successfully connect clients in crisis to services.
1. Fast Intake and Triage
Regional call centers should be available 24/7 to respond to every call received. But they need to have the documentation and resources to quickly intake each call (if further help or services are needed). The behavioral health professional should quickly be able to complete an assessment, covering:
- What led to the crisis event
- Safety and risk for the individual involved
- Resources the person in crisis has available to them at that moment
- Current prescriptions, medical history, and any inpatient hospitalizations
From there, they can coordinate with other teams to deliver the services needed, such as emergency responders or a referral to a therapist.
2. Shared Visibility Across Teams
Every partner working on a case should have access to the information they need to understand the complete picture. Behavioral health case management software increases visibility through shared tracking across:
- Responses
- Referrals
- Follow-ups
It creates a single source of truth for case notes, appointment scheduling, attendance tracking, and more. This helps call centers, mobile crisis teams, clinics, and community partners serve each person better and prevents duplicate work.
3. Closed-Loop Referrals and Warm Handoffs
A referral should not end when a phone number is given or an order is placed. Closed-loop referrals in behavioral health mean the receiving team confirms acceptance, and the sending team can see that the connection actually happened, while a warm handoff makes the transition feel supported for the patient. This is a key safeguard for high-risk behavioral health situations.
A closed-loop referral process for a crisis-to-care workflow goes like this:
- A crisis team identifies a need, such as outpatient therapy, psychiatry, housing support, or substance use treatment.
- The team sends the referral with the minimum necessary information, plus context like risk level, urgency, and preferred follow-up timing.
- The receiving organization reviews it and updates the status to something like accepted, in progress, scheduled, completed, unable to reach, or declined.
- The referring team gets updates in real time, so staff can intervene if the referral stalls or the person misses contact.
- The loop closes when the outcome is documented and the next action is assigned, such as follow-up outreach, a new referral, or discharge from active care coordination.
This process has proven to improve documentation in the referral process. For example, once Denver Health implemented a closed-loop referral system, the average rate of referral notes rose from 18.2% to 73.3%.
4. Post-Crisis Follow-up and Scheduling
After stabilization, the workflow should automatically support outreach, appointment scheduling, and continued care planning. Guidance and implementation materials emphasize proactive communication and rapid linkage to ongoing care, including follow-up within 24 hours in some crisis models. This is where relapse prevention and continuity of care really happen.
That's why it's so important to develop real-time status tracking. 988 follow-up care should include a secure, digital location where providers can see what step in the process their client is at. These dashboards should include metrics such as:
- Call volume
- Numbers of referrals
- Time-to-answer
- Abandonment rates
- Service accessibility performance
- Referral completion rates
This way, teams can always see if a problem arises before someone slips through the cracks.
5. Documentation-to-Billing Continuity
The care team should document once, in a way that supports clinical continuity, compliance, and reimbursement. Behavioral health workflows often need structured documentation that connects the crisis event, intervention, referrals, and next steps to coding and billing processes. If this link is weak, organizations lose revenue and staff spend more time re-entering the same information.
Here's an example workflow:
- Deliver service: A clinician completes the crisis visit, follow-up session, or other encounter and records details such as date, time, modality, duration, presenting issue, interventions, and response.
- Structure note to support billing: The documentation captures medical necessity, ties the service to the treatment plan, and includes the payer-specific elements required for that code.
- Coding review: The system or billing staff checks whether the documented service supports the selected CPT, HCPCS, or other billing code, and flags gaps before the claim goes out.
- Create a claim from the chart: The billing record pulls directly from the documented encounter, so staff are not retyping the same facts into a separate system.
- Validation before submission: Missing or mismatched signatures, notes, time, or medical necessity are corrected before the claim is filed.
- Submit and track claim: If the payer rejects or denies the claim, the denial reason is linked back to the documentation issue so the team can fix the source problem instead of just resubmitting blindly.
- Feedback loops improve future notes: Billing, compliance, and clinical teams review denial patterns and documentation errors to improve processes.
What Better Coordination Looks Like in Practice
Here's what the five best practices for behavioral health crisis response above look like in action:
- A person calls a behavioral health line in distress.
- The team quickly screens for urgency and dispatches a mobile crisis responder when needed.
- The team stabilizes the person in the community or through an appropriate next level of care.
- Before the encounter ends, the team schedules follow-up treatment, confirms the next provider or program, and updates the record so clinical and billing teams share the same information.
This kind of CCBHC care coordination reduces repeat intake, prevents missed follow-up, and helps ensure that the person is not left with only a referral and no next step. It also gives organizations better visibility into outcomes, because they can track whether the person was reached, stabilized, scheduled, and actually connected to care.
In short, it turns crisis response into a managed care pathway instead of a one-time intervention.
Why Disconnected Systems Fail Behavioral Health Teams
Disconnected systems fail behavioral health teams because they break the chain between assessment, coordination, follow-up, and reimbursement. They force clinicians and support staff to re-enter data, chase missing information, and reconcile conflicting records.
That slows response time in crisis situations and makes it harder to see the full patient story, which can lead to incomplete care plans or missed follow-up. The result is more administrative burden and less time for direct patient care.
And when disconnected systems fail, people and organizations suffer:
- Compromised patient safety: Incomplete or delayed information can lead to missed medication changes, duplicated work, or missed follow-up.
- Reduced staff efficiency: Manual handoffs and duplicate entry waste time and contribute to burnout.
- No continuity of care: If the next step is not visible and tracked, referrals and discharge plans are more likely to stall.
- Decreased revenue cycle performance: Documentation gaps and inconsistent data increase claim denials and rework.
Why PlanStreet Fits the Crisis-to-Care Model
Behavioral health organizations need an impact management platform like PlanStreet to help move people from crisis contact to coordinated, documented, trackable, and billable care. Our behavioral health care coordination software offers features designed specifically for organizations working with 988, CCBHCs, and other agencies.
PlanStreet helps your team:
- Track calls and intake, creating active cases with notes stored in a single, accessible location.
- Configure assessments, forms, and safety documentation to support structured triage and next-step planning.
- Follow referral workflows through completion, supporting warm handoffs and better accountability.
- Improve visibility for scheduling, notes, case details, and more, making post-crisis follow-up more manageable.
- Decrease claim denials through revenue cycle management features, including eligibility, authorizations, compliant claims, and financial reporting.
- Simplify billing through payer-specific logic, EDI file automation, increment-based billing, and batch claim submissions.
PlanStreet helps your team streamline the processes behind coordinated care, so you can focus on the people in crisis calling in.
Checklist: Questions to Help Choose Behavioral Health Crisis Coordination Software
There are a lot of different options on the market that promise improved coordination for behavioral health crisis response. While you are scheduling demos and learning more about each solution, take this checklist with you to best assess the specific needs of your organization.
Workflow fit
- Can the system support the full crisis-to-care path, from intake through follow-up?
- Can we track triage, stabilization, referral, scheduling, and closure in one place?
- Can we configure workflows for different levels of acuity or program types?
Coordination and visibility
- Does it support shared care plans, task assignments, and internal notes?
- Can it send alerts when a case needs escalation or follow-up?
- Can outside partners update referral status so we can confirm what happened?
Closed-loop referrals
- Can we send and receive referrals electronically?
- Can the system show whether a referral was accepted, scheduled, completed, declined, or missed?
- Can we track warm handoffs and follow-through after discharge?
Documentation and billing
- Can it capture medical necessity, time, service type, and discharge disposition?
- Can claims be generated from the chart or linked cleanly to the encounter?
- Does it help identify missing documentation before claims go out?
Reporting and outcomes
- What crisis metrics can we track out of the box?
- Can we measure response time, follow-up completion, referral closure, and repeat crises?
- Can reports be filtered by program, location, payer, diagnosis, or team?
Integration and interoperability
- Will it connect with our EHR, scheduling, billing, telehealth, and case management tools?
- Can it share data securely across organizations and systems?
- Can it reduce duplicate data entry across platforms?
Security and compliance
- Is it HIPAA-ready and configured for behavioral health privacy needs?
- Does it support role-based access, audit trails, and consent management?
- Can it handle sensitive notes, restricted records, and minimum necessary access?
Usability and adoption
- Is the interface simple enough for fast use in a crisis?
- How much training will staff need?
- Can it be used on desktop and mobile devices?
Scalability and support
- What implementation support, training, and customer service are included?
- How fast can the vendor respond to outages or urgent issues?
- Can the system grow with new programs, locations, or partner agencies?
Improve Behavioral Health Care Coordination With PlanStreet
PlanStreet helps your team amplify their skills, providing the tools they need to complete the no-wrong-door access workflows.
Let us show you how PlanStreet can be customized to the needs of your organization and schedule a free demo with our team today.